Physical therapy in Chevy Chase and Washington, DC for Hip
Welcome to Kesler Physical & Massage Therapy's resource with respect to recovery from Trochanteric Bursitis Surgery.
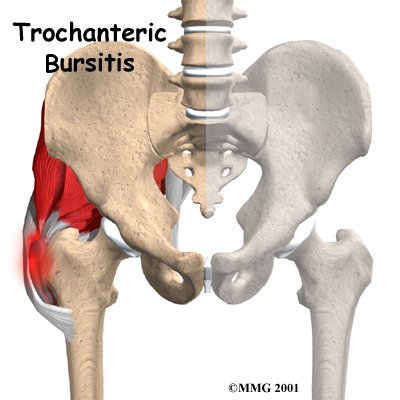
The bump of bone on the outside of the hip bone is called the greater trochanter. A fluid-filled sac, called a bursa, lies next to the greater trochanter. When the bursa in this area becomes thickened and inflamed, surgery may be needed to remove the bursa and to reduce tension on the tendon that glides over it.
This guide will help you understand:
what the surgeon hopes to achieve
what happens during the procedure
what to expect during your recovery
Anatomy
Why did my trochanteric bursa become a problem?
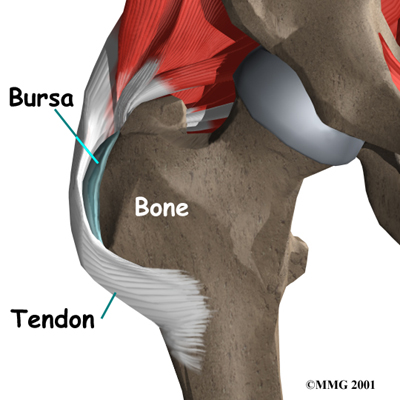
Where friction must occur between muscles, tendons, and bones, there is usually a bursa. A bursa is a thin sac of tissue that contains a bit of fluid to lubricate the area where the friction occurs. The bursa is a normal structure, and the body will even produce a bursa in response to friction.
Bursa
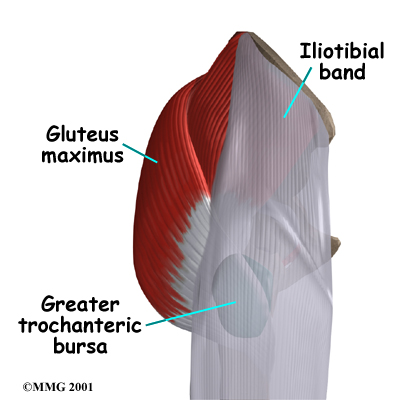
The bursa next to the greater trochanter is called the greater trochanetric bursa. The gluteus maximus is the largest of three gluteal muscles of the buttock. This muscle spans the side of the hip and joins the iliotibial band. The iliotibial band is a long tendon that passes over the bursa on the outside of the greater trochanter. It runs down the side of the thigh and attaches just below the outside edge of the knee.
Greater Trochanetric Bursa
Walking causes the gluteus maximus to pull on the tendon. If the tendon is tight, it will start to press and rub against the greater trochanteric bursa. It is unclear why the tendon becomes tight. The rubbing causes friction to build in the greater trochangeric bursa, leading to irritation and inflammation in the bursa.
View animation of rubbing on the bursa:
Friction can also start if the outer hip muscle (gluteus medius) is weak, if one leg is longer than the other, or if you run on banked (slanted) surfaces.
The primary goal of the surgical procedure for this condition is to remove the thickened bursa, to remove any bone spurs (knobby outgrowths) that may have formed on the greater trochanter, and to relax the large tendon of the gluteus maximus. Some surgeons prefer to simply lengthen the tendon a bit, and some prefer to remove a section of the tendon that rubs directly on the greater trochanter. Both procedures give good results by taking pressure off the bursa.
Preparation
What do I need to do before surgery?
Once you decide on surgery, you need to take several steps. Your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn't eat or drink anything after midnight the night before. The amount of time patients spend in the hospital varies. You will need to stay until your medical condition has stabilized and you can safely use crutches or a walker.
Before surgery begins, you will be given anesthesia. There are two basic options: a general anesthetic (one that puts you to sleep) or a regional block (one that numbs the area to be worked on). For hip surgery the most common type of regional anesthetic available is either a spinal block or an epidural block. Both of these regional blocks numb the body from the waist down.
If you choose to have a regional anesthetic, you may also be given medication to allow you to drift off to sleep if you are anxious. Either type of anesthetic can be used to perform this procedure. Be sure to discuss this with your surgeon.
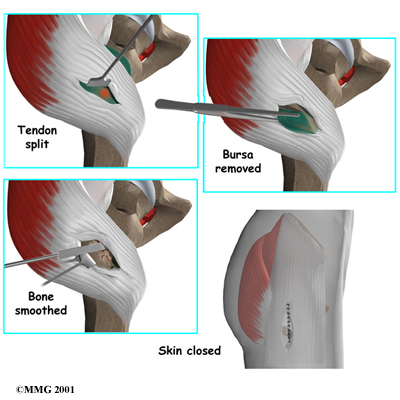
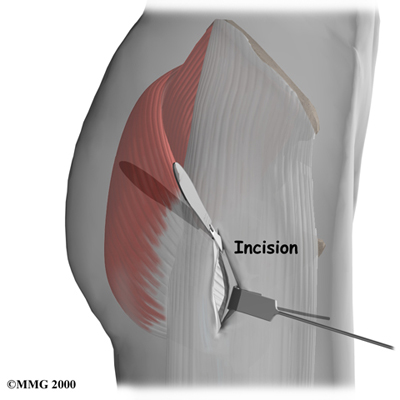
To begin the surgical procedure, an incision is made in the side of the thigh over the area of the greater trochanter. The surgeon continues the incision through the tissues that lie over the bursa.
The tendon is then split so that the trochanteric bursa and the bone of the greater trochanter can be seen. The tendon is split lengthwise. The bursa sac is removed. The bone of the greater trochanter is smoothed, and any bone spurs are removed.
At this point the tendon may be lengthened or released and not repaired. If the surgeon chooses not to repair the tendon, scar tissue will eventually heal the loose edges of the tendon. As it heals, it will be looser than before surgery, so it won't rub on the greater trochanter quite so much. The skin is closed with stitches.
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following surgery for trochanteric bursitis include:
anesthesia complications
thrombophlebitis (DVT)
infection
nerve or blood vessel injury
failure of the operation
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but it is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when the blood in the large veins of the leg forms blood clots. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible. Two other commonly used preventative measures include:
pressure stockings to keep the blood in the legs moving
medications that thin the blood and prevent blood clots from forming
Infection
Any operation carries a small risk of infection. This procedure is no different. You will probably be given antibiotics before the operation to reduce the risk of infection. If an infection occurs you will most likely need antibiotics to cure the infection. You may need additional operations to drain the infection if it involves the area around the hip.
Nerve or Blood Vessel Injury
Several smaller nerves travel in the area where the surgery is performed. It is possible to injure the nerves during surgery, but this is extremely unlikely during this type of surgery. Nerve problems may well be temporary if the nerves have been stretched by retractors holding them out of the way. It is rare to have permanent injury to the nerves, but it is possible.
Failure of the Operation
This operation may not be successful. All operations have a chance of failure, and this operation is no different. Even after going through the procedure, you may continue to have pain from trochanteric bursitis. This is clearly not the expected outcome, and the majority of patients are relieved by the procedure.
After surgery, your hip will be covered with a padded dressing. Try to avoid a lot of activity within the first week after surgery. Support your outer hip with a pillow when you sit or recline. During this time, you may also be instructed to use crutches to keep from placing weight on your hip while you stand or walk.
Keep the dressing on your hip until you return to the surgeon. Avoid getting the stitches wet. Your stitches will be removed 10 to 14 days after surgery. If your surgeon chooses to use dissolvable stitches, these will not need to be removed.
Rehabilitation after surgery can be a slow process. Although time required for recovery is different for each patient, you will probably need to attend physical therapy sessions for several weeks at Kesler Physical & Massage Therapy, and you should expect full recovery to take several months. Getting the hip moving as soon as possible is important. However, this must be balanced with the need to protect the healing muscles and tissues.
Our physical therapist may use ice and electrical stimulation treatments during your first few therapy sessions to help control pain and swelling from the surgery. Our physical therapist may also use massage and other hands-on treatments to ease muscle spasm and pain.
Our treatments include range-of-motion exercises and gradually work into active stretching and strengthening. Active therapy usually starts two to three weeks after surgery. Our physical therapist may start you on light isometric strengthening exercises. These exercises work the muscles without straining the healing tissues.
At about four weeks we may start doing more active strengthening. Exercises focus on improving the strength and control of your buttock and hip muscles. Our physical therapist will help you retrain these muscles to keep the ball of the femur moving smoothly in the socket.
Some of the exercises you'll do are designed get your hip working in ways that are similar to your work tasks and sport activities. Our physical therapist will help you find ways to do your tasks that don't put too much stress on your hip. Before your physical therapy sessions at Kesler Physical & Massage Therapy end, our physical therapist will teach you a number of ways to avoid future problems.
At Kesler Physical & Massage Therapy, our goal is to help speed your recovery so that you can more quickly return to your everyday activities. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
Kesler Physical & Massage Therapy provides services for physical therapy in Chevy Chase and Washington, DC.









 Before surgery begins, you will be given anesthesia. There are two basic options: a general anesthetic (one that puts you to sleep) or a regional block (one that numbs the area to be worked on). For hip surgery the most common type of regional anesthetic available is either a spinal block or an epidural block. Both of these regional blocks numb the body from the waist down.
Before surgery begins, you will be given anesthesia. There are two basic options: a general anesthetic (one that puts you to sleep) or a regional block (one that numbs the area to be worked on). For hip surgery the most common type of regional anesthetic available is either a spinal block or an epidural block. Both of these regional blocks numb the body from the waist down.